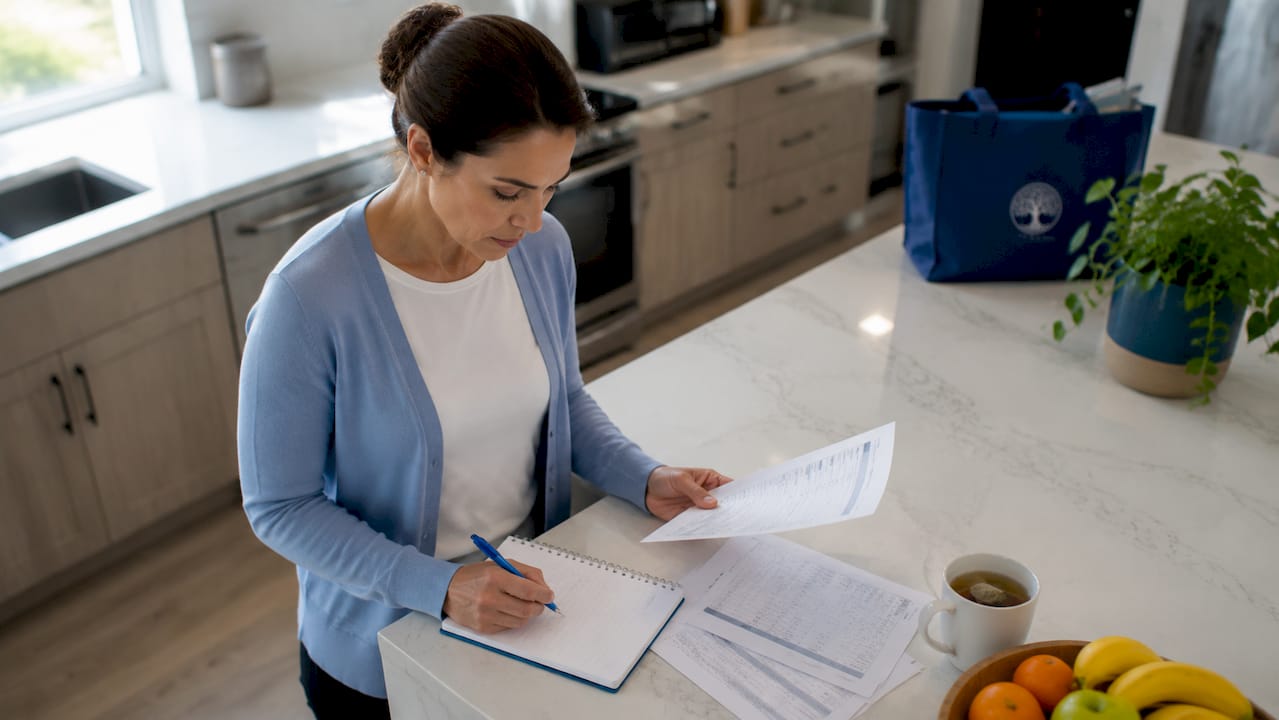
An individualized care plan is a customized treatment roadmap built around one person’s specific needs, goals, and circumstances, developed collaboratively by the patient, their family, and a licensed care team. Understanding how individualized care plans are created gives families real power in the recovery process. These plans are not generic checklists. They are structured, living documents that guide every clinical decision from the first day of treatment through discharge and beyond. In addiction recovery and mental health treatment, a well-built plan is often the difference between a patient who stays engaged and one who disengages within weeks.
What are the key steps in creating an individualized care plan?
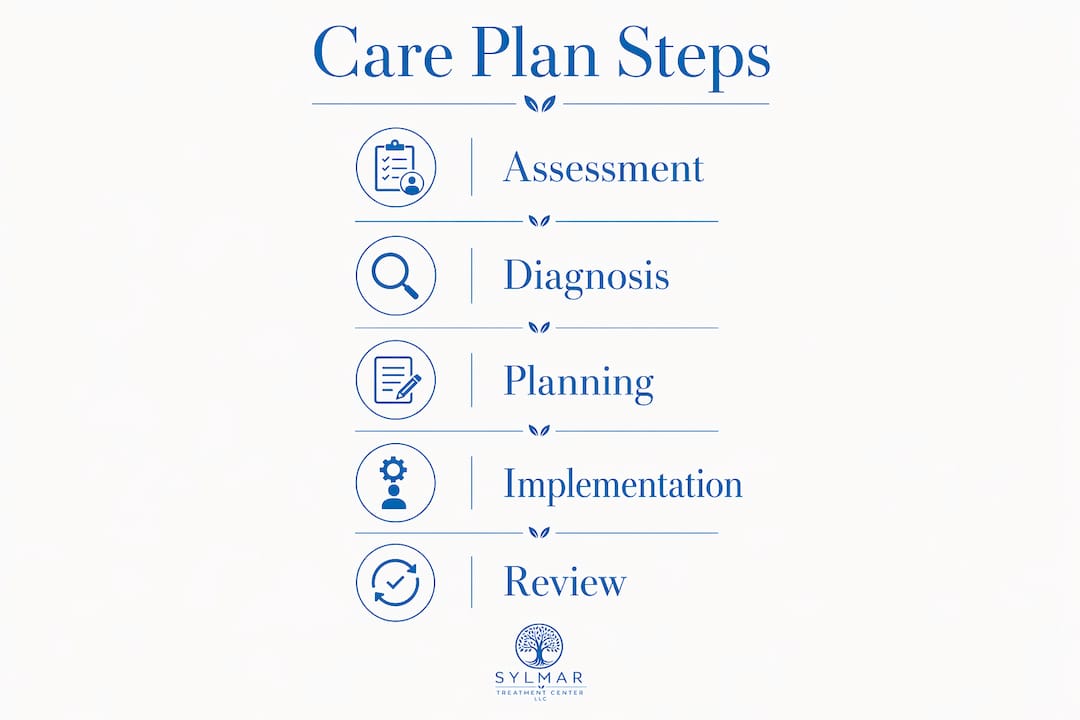
The 5-step care planning cycle is the recognized clinical framework: Assessment, Diagnosis, Planning, Implementation, and Evaluation. Each phase builds directly on the last, and skipping any one of them produces a plan that looks complete on paper but fails in practice.
-
Assessment. A licensed nurse or care coordinator conducts a comprehensive evaluation at admission, covering physical health, cognitive functioning, social history, substance use patterns, and mental health status. Tools like the Minimum Data Set (MDS) standardize this process and can be completed in person or virtually.
-
Diagnosis and needs identification. The clinical team identifies specific problems, deficits, and strengths based on assessment findings. In addiction and mental health settings, this step surfaces co-occurring disorders, trauma history, and social risk factors that shape every subsequent decision.
-
Planning. This is where SMART goals are set: Specific, Measurable, Attainable, Realistic, and Timely. A goal like “reduce alcohol use” is not a SMART goal. “Attend three group therapy sessions per week for 30 days and report cravings daily to a counselor” is. The difference in specificity directly predicts whether progress can be tracked.
-
Implementation. Interventions are assigned to specific team members with clear timelines. Medication schedules, therapy modalities, peer support activities, and family contact protocols are all documented here.
-
Evaluation. The plan is reviewed on a scheduled 90-day cycle, with additional reviews triggered by any significant change in the patient’s condition. The initial plan is typically completed within 14 to 30 days of admission.
Pro Tip: Ask the care team to walk you through each SMART goal at the first care conference. If a goal cannot be measured, it needs to be rewritten before the plan is finalized.
How does collaboration shape the individualized care plan?
Care plans are operational blueprints co-created with the patient, family, and care team. They are not a summary of a doctor’s notes. They are shared, living documents used daily by every staff member involved in treatment. That distinction matters enormously for families navigating addiction or mental health recovery.

The interdisciplinary care conference is the pivotal moment in this process. Clinicians, counselors, case managers, and family members meet to align on goals and responsibilities. This meeting transforms a template-heavy form into a personalized operational roadmap. Without it, different team members often work from different assumptions about what the patient needs.
Patient and family involvement directly increases treatment engagement and satisfaction. When patients feel heard and see their own priorities reflected in the plan, they are more likely to follow through on interventions. For families, active participation means you are not waiting for updates. You are part of generating them.
Key benefits of a collaborative approach include:
- Goals reflect the patient’s own values and recovery priorities, not just clinical defaults
- Family members understand their specific role in supporting the plan outside of treatment hours
- Care coordinators can flag conflicts between what the patient says in sessions and what family observes at home
- The plan remains accessible across the full care team, reducing miscommunication between shifts or providers
“A care plan that the patient helped write is a plan the patient is far more likely to follow.”
Pro Tip: Families should request a copy of the care plan at every conference and keep a running list of questions between meetings. The role of care coordinators includes being your point of contact between scheduled reviews.
What components make up an effective care plan?
High-quality care plans include six core components that together create clarity for everyone delivering or receiving care. The table below compares a weak plan element against a strong one for each component.
| Component | Weak version | Strong version |
|---|---|---|
| Care tasks | “Provide emotional support” | “Check in with patient at 8 AM and 4 PM daily; use motivational interviewing techniques” |
| Medication management | “Take medications as prescribed” | “Buprenorphine 8mg at 7 AM with food; counselor documents compliance in EHR by 9 AM” |
| Personal identity and preferences | Not included | “Patient prefers female counselors; responds well to art therapy; avoid group settings before 10 AM” |
| Risk management | “Monitor for relapse” | “Early warning signs include isolation and missed meals; notify care coordinator within 2 hours” |
| Measurable goals | “Improve mental health” | “Score 10 or below on PHQ-9 by day 45 of residential treatment” |
| Documentation style | Jargon-heavy clinical notes | Plain-language summaries accessible to patient and family |
The personal identity section is the most frequently omitted component in generic plans, and its absence is exactly what makes patients feel like a case number rather than a person. Lived experience, cultural background, and individual strengths belong in the plan. Identifying what a patient does well supports independence and fills gaps in care more effectively than focusing exclusively on deficits.
How are care plans maintained and updated over time?
A care plan that is written once and filed away is not a care plan. It is a liability. Plans must be reviewed every 60 to 90 days at minimum, and immediately after any significant change in health, living situation, or treatment response.
Family input keeps plans current and meaningful between formal reviews. Families often observe behavioral changes, medication side effects, or social stressors before the clinical team does. That information is clinically relevant and belongs in the plan.
Practical ways families can advocate for timely updates:
- Request a review if you notice a significant change in mood, behavior, or physical health
- Document specific observations with dates before bringing them to the care team
- Ask whether the current goals still reflect where the patient is in their recovery, not where they were at admission
- Confirm that all providers, including outpatient therapists and prescribers, have access to the most recent version
Technology now supports faster updates. Virtual assessments and digital care records allow timely plan revisions without requiring in-person appointments, which matters for patients transitioning between residential and outpatient levels of care.
Pro Tip: Before any scheduled review, write down three things that have changed since the last plan update. Bring that list to the conference. It takes five minutes and dramatically improves the quality of the revision.
How do care plans support addiction recovery and mental health treatment?
Addiction and mental health treatment require care plans that address psychological, social, and medical needs simultaneously. A plan focused only on detox misses the behavioral and relational factors that drive relapse. Tailored interventions addressing all three dimensions increase treatment adherence and produce better long-term outcomes.
Specific elements that distinguish addiction and mental health care plans from general medical plans include:
- Relapse prevention protocols with named triggers, coping strategies, and a step-by-step response plan if early warning signs appear
- Dual diagnosis coordination that integrates psychiatric medication management with substance use treatment, since co-occurring disorders require simultaneous attention
- Family involvement structures that define how and when family members participate in sessions, receive updates, and provide support at home
- Recovery-oriented goals that go beyond symptom reduction to include employment, housing stability, and social connection
- Medication management integration where prescribing decisions are documented alongside therapy goals so the full team understands the treatment rationale
For someone in residential treatment, the care plan also functions as a transition document. It captures what worked, what did not, and what the patient needs from outpatient providers to maintain progress after discharge.
Key takeaways
Individualized care plans work because they combine structured clinical assessment with personal goals, family input, and regular review cycles that keep treatment aligned with the patient’s actual progress.
| Point | Details |
|---|---|
| Five-step creation process | Assessment, Diagnosis, Planning, Implementation, and Evaluation form the standard cycle for every care plan. |
| SMART goals are non-negotiable | Goals must be Specific, Measurable, Attainable, Realistic, and Timely to track progress and adjust treatment. |
| Collaboration drives outcomes | Patient and family involvement at every stage increases engagement and makes goals personally meaningful. |
| Plans require regular updates | Reviews every 60 to 90 days, plus immediate revisions after significant changes, keep the plan clinically relevant. |
| Addiction plans address all three dimensions | Effective recovery plans integrate psychological, social, and medical needs, including relapse prevention and dual diagnosis support. |
What I’ve learned from watching care plans succeed and fail
I have reviewed hundreds of care plans across addiction and mental health settings, and the pattern is consistent. The plans that produce real results are the ones where the patient could pick it up and say, “Yes, this is about me.” The plans that fail are the ones where the patient’s name could be swapped out for anyone else’s and nothing would change.
The most common mistake families make is treating the care conference as a formality. They show up, nod, and sign. They leave without asking a single question about whether the goals reflect what their loved one actually said they wanted. That passivity is understandable. Clinical settings are intimidating. But the care plan is the one document where your voice has the most leverage, and the window to use it is narrow.
Generic plans are not just unhelpful. They are actively counterproductive. A patient who reads their own care plan and sees language that does not reflect their experience will disengage from treatment faster than almost any other factor. I have seen this happen repeatedly, and it is entirely preventable.
The other thing I would tell any family: do not wait for the 90-day review to raise a concern. If something changes, say something. The plan is supposed to reflect reality, not the reality from three months ago. Clinicians want that information. They are not always positioned to see what you see at home.
— Jim
How Sylmartreatmentcenter builds care plans that actually work
At Sylmartreatmentcenter, every patient enters a structured five-step planning process from day one. Assessments are available in person and virtually, and the first care conference happens within 14 days of admission. Families are included at every stage, from initial goal-setting through ongoing reviews.
The center’s intimate six-bed setting means care coordinators know each patient by name, not by case number. Individualized treatment programs at Sylmartreatmentcenter integrate dual diagnosis support, medication management, and relapse prevention into a single, unified plan. If you are ready to understand what a personalized plan looks like for your family, explore the full range of treatment programs or call the 24/7 admissions line today.
FAQ
What does “individualized care plan” mean in addiction treatment?
An individualized care plan is a written document that outlines a patient’s specific treatment goals, interventions, and responsibilities, built around their unique medical, psychological, and social needs. In addiction treatment, it includes relapse prevention strategies, medication protocols, and family involvement structures.
How long does it take to create a care plan after admission?
The initial assessment begins at admission, and the completed care plan is typically finalized within 14 to 30 days. The first care conference, where goals are reviewed with the patient and family, usually occurs within that same window.
How often is a care plan updated?
Care plans are reviewed on a scheduled 60 to 90-day cycle and revised immediately after any significant change in the patient’s health or circumstances. Family observations between reviews are a valid and important trigger for updates.
Can family members influence the care plan?
Yes. Family involvement directly improves care plan quality and patient outcomes. Families participate in care conferences, contribute observations, and help set goals that reflect the patient’s real-world priorities and support network.
What makes a care plan specific to mental health and addiction?
Mental health and addiction care plans include relapse prevention protocols, dual diagnosis coordination, and recovery-oriented goals that address employment, housing, and social connection alongside clinical symptom management. These elements distinguish them from general medical care plans.