
Integrated treatment is defined as simultaneous, coordinated care for both substance use and mental health disorders, delivered by a single clinical team under one unified treatment plan. This approach is the recognized gold standard for co-occurring disorders, a condition the clinical field calls “dual diagnosis.” Understanding what does integrated treatment mean matters because the model you choose directly affects whether you recover or relapse. Retention rates in integrated models reach 55–75%, compared to just 20–35% in sequential models. That gap is not a minor statistical difference. It represents thousands of people who stay in care long enough to actually heal.
What does integrated treatment mean in clinical practice?
Integrated treatment is built around one core principle: mental health and addiction are not separate problems to fix in sequence. They are intertwined conditions that must be treated at the same time, by the same team, using the same plan. Over 90% of individuals with co-occurring disorders benefit from coordinated, multidisciplinary care. That figure reflects decades of clinical research pointing in one direction.
The structural features of a genuine integrated program are specific and verifiable. A true integrated model includes all of the following:
- One multidisciplinary clinical team. Psychiatrists, addiction counselors, therapists, and case managers work together, not in separate offices or separate systems.
- A single, shared treatment plan. Every provider updates the same document. There is no version for the therapist and a different version for the prescriber.
- Medication-friendly policies. Psychiatric medications are started early, not withheld until sobriety is achieved. This is a critical departure from older models.
- Trauma-informed care standards. Trauma is treated as a clinical factor in both the addiction and the mental health disorder, not as a separate issue for later.
- Staged interventions. Care progresses from engagement and stabilization through active treatment and into relapse prevention, with the team adjusting at each stage.
Weekly interdisciplinary team meetings are required in verified integrated programs. These meetings are where the team catches gaps, adjusts medications, and keeps the treatment plan current for each patient.
Pro Tip: When evaluating any program, ask one direct question: “Does one team manage both my mental health and my addiction, using one shared plan?” If the answer is no, the program is not truly integrated.

How does integrated treatment improve outcomes vs. other models?
Sequential treatment means addressing one disorder first, then the other. Parallel treatment means treating both disorders at the same time but with separate providers who rarely communicate. Integrated treatment does neither of those things. It treats both disorders simultaneously with full team coordination.
The clinical reality is straightforward. Mental health disorders and addiction feed each other. Untreated depression drives alcohol use. Untreated trauma fuels opioid dependence. When you treat only one side of that equation, the untreated side pulls the patient back. Sequential models create a revolving door. Parallel models create fragmented care where the left hand does not know what the right hand is doing.
The outcome data reflects this directly:
| Treatment Model | 6-Month Retention | Symptom Improvement | Team Coordination |
|---|---|---|---|
| Integrated | 55–75% | Durable, concurrent | Single unified team |
| Sequential | 20–35% | Delayed, one disorder at a time | Separate providers, sequential handoffs |
| Parallel | Moderate | Inconsistent | Separate providers, minimal communication |
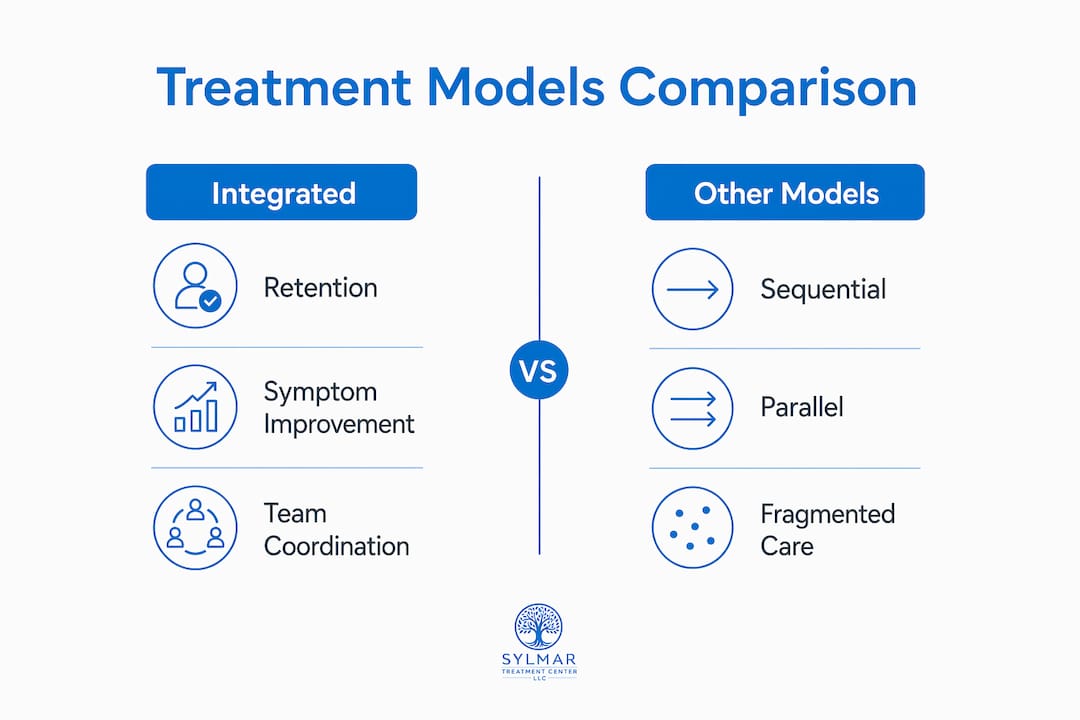
Integrated treatment produces more durable symptom improvement than either alternative model. Durability matters because recovery is measured in years, not weeks. A patient who improves quickly but relapses at six months has not recovered. Integrated care is specifically designed to prevent that pattern.
Pro Tip: Ask any treatment center for their 6-month retention data. Programs with genuine integrated care will have this number. Programs that do not track it are telling you something important about their model.
What therapy approaches are used in integrated treatment?
Integrated treatment draws from a specific set of evidence-based therapies, each chosen because it addresses both mental health symptoms and addictive behaviors at the same time. Trauma-informed care is a fundamental component of every credible integrated program, not an optional add-on.
The core therapies used in integrated treatment include:
- Cognitive-behavioral therapy (CBT). CBT targets the thought patterns that drive both depression and substance use. A patient learns to identify triggers for anxiety and for cravings within the same session.
- Dialectical behavior therapy (DBT). DBT builds emotional regulation skills. Patients with borderline personality disorder or severe trauma histories use DBT to manage the emotional volatility that often precedes relapse.
- Motivational interviewing (MI). MI addresses ambivalence about change. Many patients entering treatment are not fully committed to sobriety or to psychiatric medication. MI resolves that ambivalence without confrontation.
- EMDR (Eye Movement Desensitization and Reprocessing). EMDR processes traumatic memories that sit at the root of both PTSD and addiction. It is one of the few therapies with strong evidence for both conditions simultaneously.
- Mindfulness-based interventions. Mindfulness reduces the reactivity that drives both anxiety episodes and cravings. Programs use it as a daily skill, not just a weekly group exercise.
A typical integrated treatment plan combines two or three of these therapies with psychiatric medication management and structured family involvement. For example, a patient with major depression and alcohol use disorder might receive CBT three times per week, attend a family therapy session biweekly, and work with a psychiatrist on antidepressant dosing, all coordinated through one individualized care plan updated by every provider on the team.
Family involvement is not peripheral in integrated treatment. Family members are educated about both the mental health disorder and the addiction, because family dynamics often reinforce one or both conditions. Bringing the family into the treatment plan reduces that risk.
What misconceptions make it harder to find real integrated care?
The biggest misconception is that “dual diagnosis” and “integrated treatment” mean the same thing. They do not. “Dual diagnosis” describes the condition. “Integrated treatment” is the specific clinical model used to treat it. A program can accept patients with dual diagnoses and still use a sequential or parallel model. Accepting dual diagnosis patients does not make a program integrated.
The second major misconception is that mental health must be stabilized before addiction treatment can begin. This belief comes from the legacy of sequential treatment, which dominated the field for decades. The clinical evidence now contradicts it. Withholding psychiatric medication until a patient achieves sobriety delays stabilization and increases relapse risk. Integrated treatment starts both tracks on day one.
Patients can take concrete steps to verify whether a program is truly integrated:
- Ask about team structure. Request the names and roles of every provider who will work on your case. If they are employed by different organizations, the model is parallel, not integrated.
- Request the treatment plan format. A genuine integrated program uses one document, updated by all providers. Ask to see a sample or template.
- Confirm meeting frequency. Unified clinical teams meet weekly to review each patient. Ask how often your team will meet and who attends.
- Ask about medication policy. Find out whether psychiatric medications can be started before full sobriety is achieved. A “no” signals a sequential mindset.
- Verify accreditation. DHCS licensure and Joint Commission accreditation are external checks that programs meet defined clinical standards. These credentials are publicly verifiable.
Organizational barriers like cultural resistance and care fragmentation prevent many programs from achieving true integration even when they intend to. Patients who ask these questions protect themselves from programs that use the language of integration without the structure.
Key Takeaways
Integrated treatment is the only model that treats co-occurring disorders simultaneously, with one team and one plan, producing retention rates up to three times higher than sequential care.
| Point | Details |
|---|---|
| Core definition | Integrated treatment means one team, one plan, treating addiction and mental health at the same time. |
| Retention advantage | Integrated models reach 55–75% retention at six months vs. 20–35% in sequential programs. |
| Therapy mix | CBT, DBT, motivational interviewing, EMDR, and mindfulness are the primary evidence-based tools. |
| Verification step | Confirm unified team meetings, a shared treatment plan, and medication-friendly policies before enrolling. |
| Key distinction | Dual diagnosis is the condition; integrated treatment is the clinical model that addresses it effectively. |
Why the siloed system still fails too many patients
I have spent years watching people cycle through treatment programs that looked integrated on paper but were not in practice. The therapist worked in one building. The prescriber was in another. The case manager got a fax once a week. Nobody called it sequential. They called it “coordinated care.” The patient paid the price.
The historic separation of mental health and addiction services is the single biggest structural failure in American behavioral health. These two fields developed separately, trained separately, and billed separately for decades. That history does not disappear because a program puts both words on its website.
What actually changes outcomes is the meeting. The weekly interdisciplinary team meeting where the psychiatrist, the addiction counselor, and the therapist sit in the same room and talk about the same patient. That meeting is where integration happens. Without it, you have parallel care with better marketing.
My advice to anyone evaluating a program is simple. Do not ask whether they treat dual diagnosis. Ask when the team last met to discuss a patient’s progress across both disorders. The answer tells you everything. Successful integrated care requires system-level alignment, not just good intentions from individual clinicians.
— Jim
Integrated treatment programs at Sylmartreatmentcenter
Sylmartreatmentcenter operates with a unified clinical team that addresses both substance use and co-occurring mental health disorders through coordinated, evidence-based care. Every patient receives a custom treatment plan built by psychiatrists, addiction counselors, and therapists working together from day one.
The center’s dual diagnosis programs combine psychiatric medication management, trauma-informed therapy, and family involvement in a six-bed residential setting that allows for genuinely personalized attention. DHCS licensure and Joint Commission accreditation confirm that the clinical standards match the model. Patients and families can reach the admissions team any time through 24/7 support. To review the full range of treatment programs available, including residential and individualized care options, visit the Sylmartreatmentcenter programs page.
FAQ
What does integrated treatment mean for addiction?
Integrated treatment for addiction means one clinical team treats both the substance use disorder and any co-occurring mental health condition at the same time, using a single shared treatment plan. This model produces retention rates of 55–75% at six months, compared to 20–35% in sequential programs.
What is the difference between dual diagnosis and integrated treatment?
Dual diagnosis describes the condition of having both a mental health disorder and a substance use disorder. Integrated treatment is the specific clinical model designed to treat that condition effectively, using one team and one coordinated plan.
How does integrated treatment work in practice?
A multidisciplinary team including a psychiatrist, addiction counselor, and therapist shares one treatment plan and meets weekly to coordinate care. Therapies like CBT, DBT, and motivational interviewing address both disorders simultaneously rather than in sequence.
What are the benefits of integrated treatment over sequential care?
Integrated treatment produces higher retention, more durable symptom improvement, and lower relapse rates than sequential or parallel models. The primary benefit is that neither disorder is left untreated while the other is being addressed.
How do I know if a program is truly integrated?
Verify that one team manages both disorders, that all providers update a single shared treatment plan, and that the team meets weekly. Programs with unified clinical teams and medication-friendly policies from day one meet the standard for authentic integrated care.