Starting Detox in a Six-Bed Facility: A Safety Guide

Starting detox with a six-bed facility means choosing an intimate, medically monitored setting where clinical staff know your name, your history, and your withdrawal pattern from day one. The industry term for this level of care is medically monitored inpatient detoxification, defined by the American Society of Addiction Medicine as a structured environment with 24-hour nursing and physician availability. Small detox facilities like this sit at the intersection of clinical rigor and personal connection. Sylmartreatmentcenter operates exactly this model, holding both a DHCS license and Joint Commission accreditation, which means every protocol meets state and national standards. This guide walks you through what to expect, what to prepare, and what to watch out for.
What medical and regulatory requirements must a six-bed detox facility meet?
ASAM Level 3.7 defines the standard for medically monitored inpatient detox. It requires 24-hour nursing coverage, physician availability, medication administration protocols, and structured transition planning at discharge. A six-bed detox center that meets this standard is not simply a comfortable house. It is a licensed clinical program with documented care protocols.
Regulatory requirements vary by state, but California sets one of the most detailed frameworks. California DHCS licensing requires facilities to complete a formal application (DHCS Form 6002), pass a fire inspection, obtain zoning approval, and document bed count before receiving a license. These steps apply to any program providing clinical services, including detox, counseling, or treatment planning.
There is one important exception. Small homes under six beds that offer only housing and peer support without clinical services may be exempt from DHCS licensing. The moment a facility adds detox monitoring, medication management, or structured treatment planning, full licensure is required. Local zoning ordinances still apply regardless of exemption status.
- ASAM Level 3.7 compliance: Confirms 24-hour nursing and physician-directed care protocols are in place.
- DHCS license: Verifies the facility has passed California’s application, fire, and zoning review process.
- Joint Commission accreditation: An independent quality check that goes beyond state minimums.
- Bed count documentation: Required for licensing and directly affects staffing ratios.
- Local zoning approval: Applies to all facilities, licensed or exempt.
Pro Tip: Ask any facility you consider for their DHCS license number and Joint Commission accreditation status before admission. Both are publicly verifiable, and a legitimate program will share them without hesitation.
What do you need before starting a detox program at a small facility?
Preparation before admission directly affects how safely your first hours go. Pre-admission phone screenings collect your substance type, usage patterns, withdrawal history, current medications, and any co-occurring mental health conditions. That information shapes your detox plan before you walk through the door.
The intake assessment is not a formality. Clinical staff use it to anticipate your withdrawal timeline, identify high-risk complications, and prepare medications in advance. Patients who share complete histories, including prior seizures or delirium tremens, receive more targeted care from the first hour.
What to bring when you arrive:
- Government-issued ID and insurance card for admission processing.
- Prescription medications in original bottles so staff can verify dosages.
- A small personal bag with comfortable clothing, toiletries, and any comfort items the facility permits.
- Emergency contact information for at least one trusted person.
Phone use is often restricted during the first 24–48 hours. That restriction is not punitive. It protects your ability to focus on medical stabilization without outside stressors interfering. Review the facility’s communication policy before arrival so family members know what to expect. A resource like this detox packing guide from Sylmartreatmentcenter covers the specifics in detail.
Pro Tip: Write down your full substance use history, including dates, amounts, and any previous withdrawal complications, before your intake call. Verbal recall under stress is unreliable, and a written record helps clinicians build a safer plan.
Step by step: What happens during detox in a six-bed facility?
The detox process follows a predictable clinical sequence, even though your personal experience will feel anything but predictable. Understanding the timeline reduces fear and helps you cooperate with the medical team.

1. Arrival and initial assessment (hours 0–4) Staff record your vital signs, including blood pressure, heart rate, respiratory rate, temperature, and oxygen saturation. They document the time since your last substance use. This baseline determines your starting medication protocol.
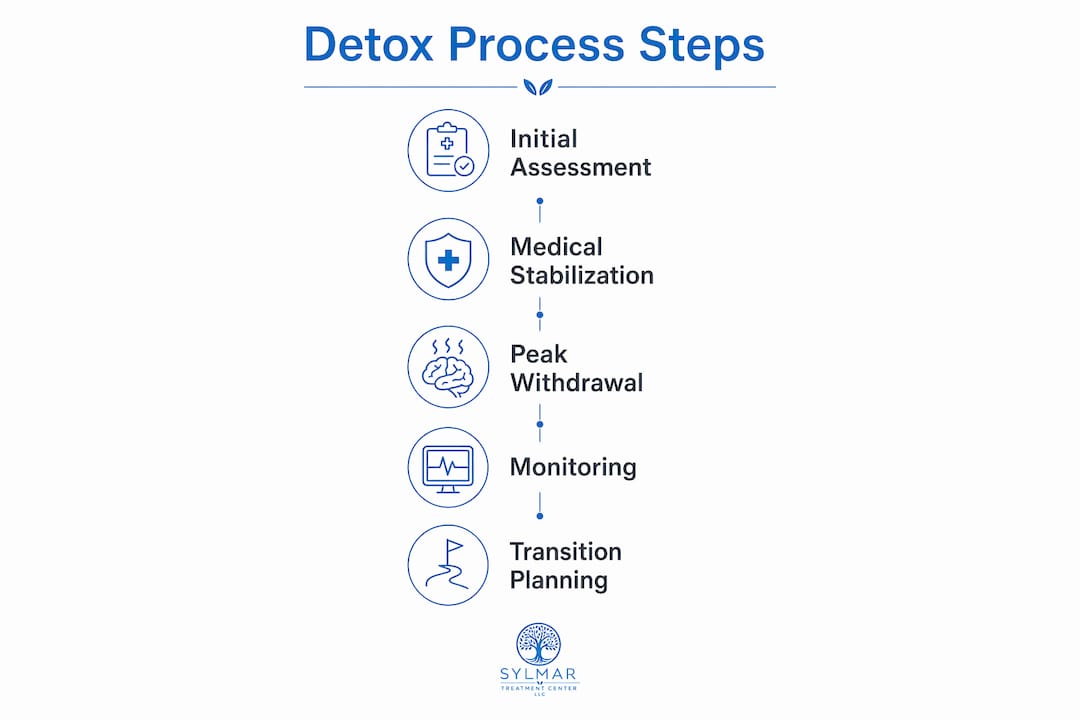
2. Medical stabilization (hours 4–24) The first 24 hours focus on intensive stabilization with frequent vital-sign checks. Medications are titrated based on your response. Rest is the primary activity. Expect to sleep, feel uncomfortable, and have nurses check on you regularly.
3. Peak withdrawal monitoring (hours 24–96) Alcohol withdrawal symptoms peak 24–72 hours after last use. Dangerous complications like delirium tremens can emerge 48–96 hours in. This is the highest-risk window, and continuous clinical monitoring is non-negotiable during it. Symptoms can include sweating, tremors, nausea, elevated blood pressure, rapid heartbeat, hallucinations, and seizures.
4. Stabilization and light programming (days 4–7) Once withdrawal stabilizes, early detox shifts from pure monitoring to brief educational groups and counselor check-ins. Therapy is minimal at this stage. The clinical team is still the primary focus, not group sessions.
5. Discharge planning begins Transition planning starts before you feel ready. Staff coordinate your next level of care, whether residential treatment or intensive outpatient, so there is no gap between detox and continued recovery support.
“The first few days of detox are not about insight or therapy. They are about keeping you safe while your body adjusts. Rest is part of the treatment.”
In a six-bed setting, rooming arrangements are typically private or shared between two patients. That privacy matters during peak withdrawal, when physical symptoms are at their worst and personal dignity is already under pressure.
How does a six-bed detox facility ensure continuity of care after detox?
Detox is not treatment. It is the medical gateway to treatment. A facility that discharges you without a confirmed next step has completed only half the job.
A 2014 analysis published in the Journal of Substance Abuse Treatment confirms that direct transfer from detox to residential or intensive outpatient care produces significantly lower relapse rates at both 30 and 90 days compared to discharge without follow-up planning. That finding has shaped how responsible detox programs operate. The warm handoff, a direct referral with active coordination between the detox team and the receiving program, is now a clinical best practice.
Ask these questions before choosing any small detox facility:
- Does the facility have established referral relationships with residential programs?
- Will a staff member actively coordinate my transfer, or will I be handed a list of phone numbers?
- How far in advance does transition planning begin?
- Does the facility offer individualized treatment programs or refer to programs that do?
| Facility type | Transition planning approach |
|---|---|
| Strong six-bed detox center | Active warm handoff, confirmed placement before discharge |
| Weak six-bed detox center | Discharge paperwork with referral list, no active coordination |
| Large hospital detox unit | Discharge planner assigned, but caseloads may limit personal follow-up |
| Unlicensed peer support home | No clinical transition planning capability |
Pro Tip: Ask specifically whether the facility will confirm your next placement before your discharge date, not after. A confirmed bed in a residential program on discharge day is the standard you should expect.
What common mistakes should you avoid when starting detox with a small facility?
Choosing a small detox facility based on aesthetics alone is the most common and most dangerous mistake. A comfortable house with attentive staff but no physician availability cannot safely manage alcohol or benzodiazepine withdrawal. Those withdrawals can be fatal without proper medical intervention.
Patients frequently misread the early detox experience as neglect. Clinicians prioritize safety via close medical monitoring and medication titration during peak withdrawal, not therapy sessions. Expecting group counseling on day two sets you up for frustration and erodes trust in staff who are actually doing their jobs correctly.
Common mistakes to avoid:
- Choosing comfort over clinical capability. A beautiful setting with inadequate medical staffing is a liability, not an asset.
- Withholding substance use history. Incomplete histories lead to undertreated withdrawal and preventable complications.
- Expecting therapy during peak withdrawal. The first 72 hours are for medical stabilization, not insight work.
- Skipping license verification. Any facility providing clinical detox services in California must hold a DHCS license. Verify it before admission.
- Leaving without a confirmed next step. Detox without a transition plan dramatically increases relapse risk.
Emotional preparation matters as much as practical preparation. Withdrawal is physically and psychologically intense. Patients who understand what is coming, including the discomfort, the restricted phone access, and the clinical focus of early days, cope significantly better than those who arrive with unrealistic expectations.
Key takeaways
A six-bed detox facility provides the safest, most personalized start to recovery when it holds proper licensure, meets ASAM Level 3.7 standards, and actively coordinates your transition to ongoing treatment.
| Point | Details |
|---|---|
| Verify licensure before admission | Confirm DHCS license and Joint Commission accreditation to ensure clinical standards are met. |
| Prepare a complete substance history | Accurate intake information allows staff to anticipate withdrawal risks and prepare medications in advance. |
| Expect monitoring before therapy | Peak withdrawal requires medical stabilization first; structured programming begins only after symptoms stabilize. |
| Demand a warm handoff | Confirm your next placement before discharge day to reduce relapse risk significantly. |
| Choose clinical capability over comfort | Physician availability and 24-hour nursing matter more than facility aesthetics when withdrawal is life-threatening. |
What I’ve learned from watching patients choose small detox facilities
Small facilities get two things right that large hospital units rarely do: staff actually learn who you are, and the environment does not feel institutional. Those are real advantages. But I have also watched patients choose a six-bed home based entirely on photos and a friendly intake call, only to discover the facility had no physician on call and no plan for what came after discharge.
The patients who do best in small detox settings are the ones who ask hard questions before they arrive. They want to know the nurse-to-patient ratio. They ask which physician covers overnight emergencies. They ask what happens on discharge day if their residential bed is not ready. Those questions feel uncomfortable to ask, and they are exactly the right ones.
Managing expectations is not just a clinical nicety. Patients who understand that the first three days involve more monitoring than conversation, more medication than therapy, and more discomfort than relief, those patients cooperate with their care team instead of fighting it. Cooperation during peak withdrawal is a clinical advantage. It keeps you safer.
The marketing language around small detox facilities often emphasizes community and connection. Those things are real and they matter. But they come after the medical work is done. Prioritize safety first. The community follows naturally in a well-run six-bed setting.
— Jim
Sylmartreatmentcenter’s medical detox programs for personalized care
Sylmartreatmentcenter operates a licensed six-bed inpatient detox program with 24/7 nursing coverage and physician oversight built into every admission. The center holds both a DHCS license and Joint Commission accreditation, which means the clinical standards described in this article are not aspirational. They are operational.
Sylmartreatmentcenter’s medical detox program includes individualized care plans, comprehensive intake assessments, and active transition planning to residential treatment or other appropriate levels of care. The center also addresses co-occurring mental health conditions through its dual diagnosis support program. If you are ready to take the first step, Sylmartreatmentcenter’s admissions team is available around the clock to answer your questions and begin the intake process.
FAQ
What is ASAM Level 3.7 and why does it matter for detox?
ASAM Level 3.7 is the clinical standard for medically monitored inpatient detoxification, requiring 24-hour nursing and physician availability. It matters because alcohol and benzodiazepine withdrawal can be fatal without continuous medical oversight.
How long does detox in a six-bed facility typically last?
Most medically supervised detox programs last 5–10 days depending on the substance, severity of dependence, and individual withdrawal response. Alcohol withdrawal symptoms peak at 24–72 hours and dangerous complications can arise up to 96 hours after last use.
Do small detox facilities need to be licensed in California?
Any facility in California providing clinical detox services, including medication management or treatment planning, must hold a DHCS license. Small homes under six beds offering only housing and peer support may qualify for an exemption, but local zoning rules still apply.
What should I ask a six-bed detox center before admission?
Ask for their DHCS license number, their physician coverage model, their nurse-to-patient ratio, and how they coordinate transition to the next level of care. A facility that cannot answer these questions clearly is not ready to manage your withdrawal safely.
Is therapy available during the first days of detox?
Structured therapy is minimal during peak withdrawal because clinical monitoring and medication take priority over group sessions in the first 72 hours. Brief counselor check-ins may occur, but formal programming typically begins only after withdrawal stabilizes.